


Can the Shingles Vaccine Prevent Dementia?
Signs point to yes (at least for women).

You may have seen headlines about a fascinating new study in Nature suggesting that the shingles vaccine may lower the risk of dementia.
But is this news too good to be true? (It’s been known to happen…)
TL;DR: The study provides convincing evidence that the shingles vaccine reduces the risk of dementia- but only in women.
📌 Key strengths: The researchers used a natural experiment to mimic a randomized trial, taking advantage of a real-world policy change. They also performed many checks to strengthen their claim of cause and effect.
📌 Key caveat: The paper underplays a major finding- the effect is only seen in women, and this deserved more transparency and attention.
How could a vaccine protect against dementia?
There’s growing interest in the role of infections in cognitive decline and dementia, especially herpesviruses like varicella-zoster virus (VZV), the cause of chickenpox and shingles.
Unlike most viruses, herpesviruses persist in the body for life. Your immune system works in the background to keep them in check, but they can reactivate during stress or other immune suppression, possibly increasing dementia risk via neuroinflammation or contributing to accumulation of amyloid plaques in the brain.
I’ve been fascinated with infections and the brain for many years and worked a bit in this area, finding suggestive links between the herpesviruses (HSV-1) and cytomegalovirus (CMV) and worse cognition in older adults. But our studies and others were only suggestive of a link, and couldn’t prove cause and effect. Links between infections and chronic disease are hard to prove because we can’t randomly assign infections, and exposure to infections is correlated with many social factors that may “confound” the relationship. For example, even in the US, kids from families with lower incomes get exposed to common viruses more often than more financially advantaged kids. These kids may grow up to have a higher risk of dementia for many reasons (less education, more chronic stress) that have nothing to do with these infections.
When bureaucrats do the randomizing
That’s what makes this new study exciting- it uses a natural experiment to overcome this fundamental analytical challenge. Specifically, the researchers took advantage of the introduction of the shingles vaccine in Wales in 2013.
Due to limited supply, only people under 80 were eligible for the new shingles vaccine. This meant that people born right after the cut-off date of September 2, 1933 had access to the shingles vaccine while those born right before the cut-off did not, creating two groups that are nearly identical except for vaccine access.
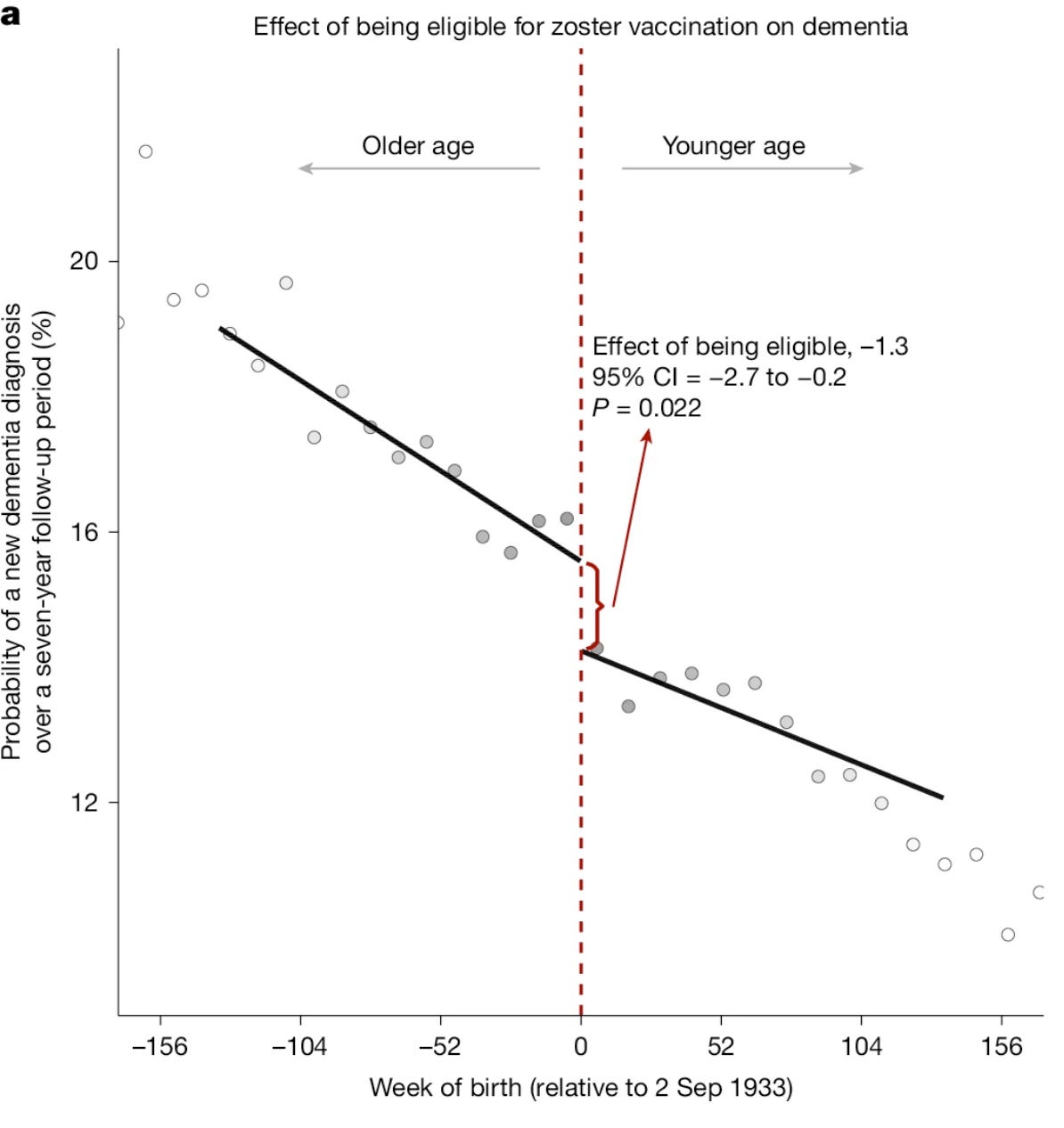
This kind of design is called a regression discontinuity design (RDD). When it works, we can more confidently believe that differences in the outcome (dementia) are caused by the treatment (shingles vaccine), since this is the only thing that was different across groups. You can see this “discontinuity” below:

Source: Eyting, M., Xie, M., Michalik, F. et al. A natural experiment on the effect of herpes zoster vaccination on dementia. Nature (2025). Figure 1A.
This figure shows that the premise of the “experiment” looks good—people born right after the cut-off were much more likely to receive the vaccine (47.2%) compared to people born right before (0.01%). The “experiment” also worked as expected with those born after the cut-off less likely to get shingles over the next few years (yay, vaccines!).
Feeling good about the validity of this experiment, the researchers linked up medical records and followed people for seven years. The main outcome of interest was a new diagnoses of dementia- people who already had dementia at baseline were excluded.
The moment of truth
Using this policy cut-off as a stand-in for randomization, the study found that the shingles vaccine reduced dementia risk by about 3.5 percentage points, a 20% relative reduction from a baseline probablity of around 17.5%. (The effect size below is smaller because it is the effect of being eligible for vaccination, but not everyone got the vaccination).
Source: Eyting, M., Xie, M., Michalik, F. et al. A natural experiment on the effect of herpes zoster vaccination on dementia. Nature (2025). Figure 3.
The authors explore a few potential mechanisms. Reassuringly, they find no evidence that people who get shingles are more likely to be diagnosed with dementia simply due to more contact with the health system. Overall, they find suggestive but not definitive evidence that the vaccine prevents dementia through suppression of viral reactivation and overall immunomodulation.
Needless to say, this result is exciting. While we’d love to prevent dementia entirely, a 20% reduction in risk for a simple intervention not received until almost age 80 is quite remarkable. Since the brain changes associated with dementia develop over long periods of time, it’s feasible that earlier intervention could have an even bigger impact (but this should be tested).
Kicking the tires…hard.
With natural experiments, the burden of proof is on researchers to rule out other explanations. The authors (likely prompted by some tough reviewers) took this charge seriously. Among many checks they showed:
✅ No difference in dementia for people born around September 2nd in years without the change in vaccine policy.
✅ No pre-vaccine differences in dementia diagnosis around the Sept cut-off.
✅ No differences in unrelated outcomes (heart attacks, cancer, diabetes, meds) across groups.
✅ No meaningful difference in education levels, addressing concerns that the September 2nd cut-off might relate to school start dates and schooling duration, an important point raised by
.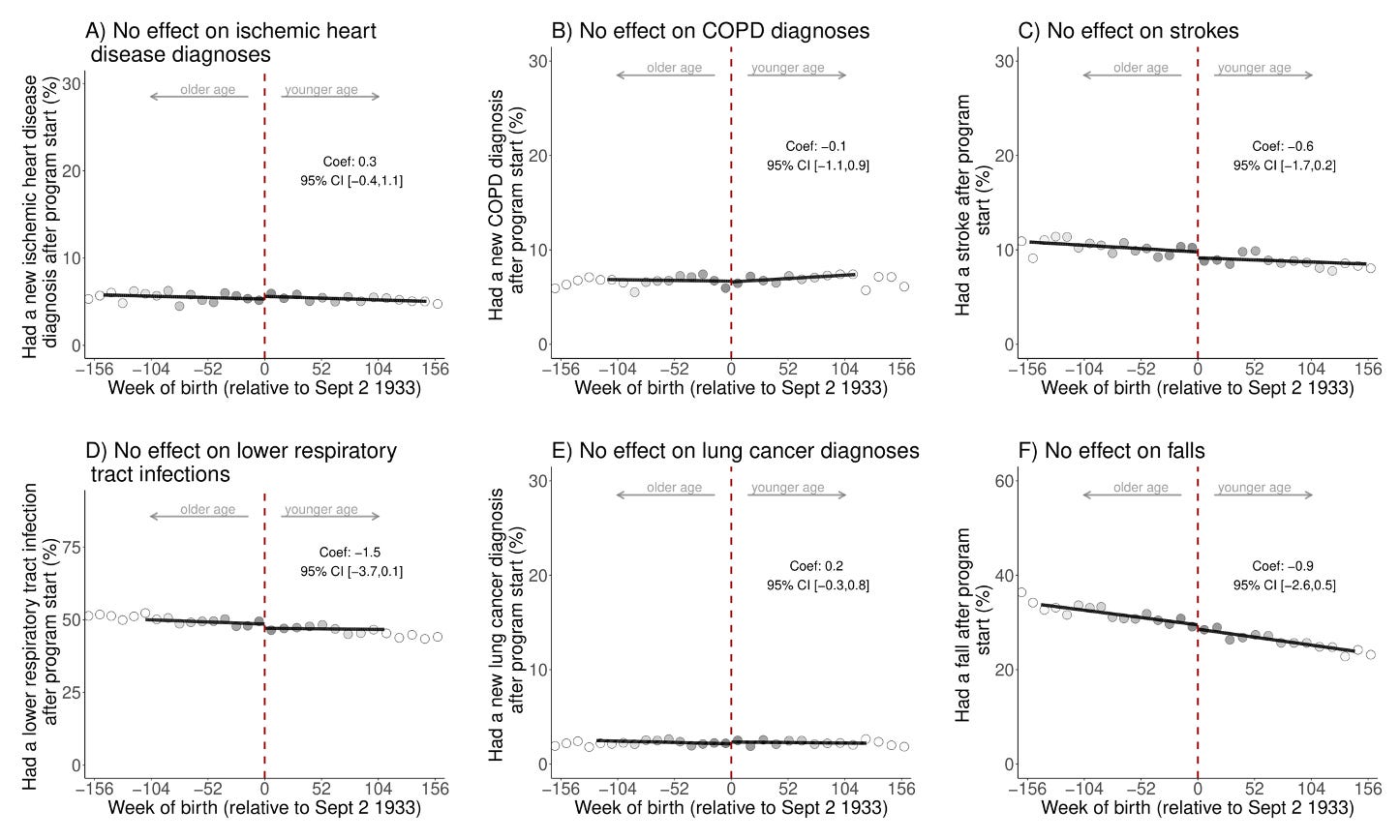
Source: Eyting, M., Xie, M., Michalik, F. et al. A natural experiment on the effect of herpes zoster vaccination on dementia. Nature (2025). Supplemental Materials.
In my view, these checks go a long way towards shoring up the key assumption that the change in vaccine policy, not any other factors, explains the differences in dementia.
Still, no study is perfect…
As much as I was impressed by this paper, I was bothered by one thing: the key finding applies only to women, but this fact is somewhat buried in the paper.
In the title, abstract, and most of the results, the benefit of vaccination is implied to apply to everyone. The authors state that “women benefitted more than men,” which to me implies there is a benefit for men. But the results show no effect in men-not just statistically imprecise, but close to zero:

Source: Eyting, M., Xie, M., Michalik, F. et al. A natural experiment on the effect of herpes zoster vaccination on dementia. Nature (2025). Figure 5.
The authors mention possible biological reasons for this sex difference (e.g., differences in the immune response to vaccines and the pathology of dementia), but the topic deserved more attention. Given the strong results only for women, I would have liked to see the robustness checks separately for men and women. This would make me more confident that evidence for these alternative explanations was not obscured by looking at men and women combined. While these sex-specific effects are not great news for men, the silver lining is that the effect size for women was even larger than it seemed, since men were bringing down the overall average.
Other dementia epidemiologists encouraged caution around these results when they were first published as a pre-print, partly because of the puzzle of these sex-specific results. Dementia also takes a long time to develop, so understanding how an effect could be seen over a relatively short time period is important. The authors replicated their findings in England and Wales, where a similar birthday cut-off was used for vaccine roll-out. While this replication increases our confidence in the results, it will be important to replicate in other settings and ideally follow-up participants in shingles randomized clinical trials to measure their cognitive function and risk of dementia over time.
Overall these results are really encouraging, and hopefully move the science of infections and dementia into the mainstream where it can get in-depth attention. Given the lack of effective treatments for dementia, the potential for prevention through vaccination or treatment of infections could be huge.
Do these results apply to the newer shingles vaccine, Shingrix?
This study looked at the introduction of the shingles vaccine Zostavax, a live attenuated vaccine that has since been replaced in most places by Shingrix, a non-live recombinant vaccine that provides better protection against shingles. Luckily, another recent study used a similar natural experiment in the US of the rapid switch from Zostavax to the newer Shingrix vaccine, finding that people getting Shingrix rather than the older version of the vaccine had a lower risk of developing dementia. This is good news and consistent with a mechanism of protection against dementia by suppressing viral reactivation, for which Shingrix is more effective.
Bottom line: Getting the shingles vaccine is a no-brainer
Imagine a vaccine that protects you from a painful, debilitating illness and may reduce your risk of dementia. Thanks to (federally-funded) SCIENCE, that day may already be here. If you are eligible, go get your shingles vaccine! (That means you too men, since avoiding shingles is reason enough and the chance of a dementia benefit is a bonus.)
Pictured below, my Nerdy glee after my first Shingrix dose last fall…

Stay well-
Jenn
Excellent article, thanks
Thanks for the article! One question, if the effect on reducing dementia among women is going through the prevention virus reactivation, do you think that anti-viral drugs could help people that already have symptoms of dementia like amyloid plaques in their brain fluid? Do you know of any studies on this?